

Category Archives: What You Need To Know
2016 Update: When should women start regular mammograms? 40? 50? And how often is “regular”?
Diana Zuckerman, Ph.D. and Anna E. Mazzucco, Ph.D.
Updated 2016
In recent years, there has been a growing concern that annual mammograms starting at age 40 may do more harm than good for many women. That is why the U.S. Preventative Services Task Force, an expert group that reviews the latest research findings, recommends that mammography screening for most women start at age 50 rather than 40, and that the frequency be every two years (instead of annually) through the age of 74.
The Task Force is widely used as a gold standard for determining medical treatment and screening. In this case, they recommended raising the age to 50 after the American College of Physicians recommended the same thing, and they also recommended that women continue to undergo mammograms until age 74. They say that there is no evidence of what the benefits might be for women 75 and older.
For many years, the American Cancer Society (ACS) recommended annual mammograms starting at age 40, but in October 2015, they issued new recommendations that moved in the direction of those of the medical experts. They now recommend that women at average risk of breast cancer start mammography at 45, that they undergo annual mammograms from 45-54, and continue to undergo mammography every other year after that. Experts do not recommend MRIs for screening women of average risk, but clinical studies are being done to determine whether they should be.
So what is best for you?
A key reminder: these recommendations are for screening mammograms. Mammograms are still needed at almost any age if a lump is found. The mammography recommendations also do not apply to all women, only for the average woman. Experts agree that women at especially high risk of breast cancer, such as those with mothers or sisters who had breast cancer, may want to start mammograms between the ages of 40 and 50 or in rare cases, even earlier.
The bottom line is that mammograms help detect breast cancer earlier. However, like most medical procedures, there are risks as well as benefits.
Whether to start at age 50, or 40, or even earlier depends on several different factors.
For most women, who are not at especially high risk of breast cancer, regular mammograms can start at age 50. Or, to be cautious, a woman can get one mammogram earlier (around age 45) and then if it is normal, wait until she is 50 for her next mammogram. This is the advice that the National Center for Health Research and their Cancer Prevention and Treatment Fund have been giving since 2007.
Women at higher risk of breast cancer should not wait until they are 50 to have regular mammograms. Please remember that the higher age– 50– is only a guideline (not a strict rule) and only for screening women with no symptoms and not at high risk of breast cancer. In addition, if a woman finds a lump on her breast, a mammogram is still very important, regardless of the woman’s age. For a woman at high risk of breast cancer because of her family history or environmental exposures, regular screening before age 50, or even before age 40, may be a very good idea.
Women who are carriers of the BRCA genetic mutation were previously recommended to begin yearly mammograms between ages 25-30, since this mutation puts them at much higher risk of getting breast cancer. Newer studies have found that starting yearly mammograms before age 35 has no benefit and may instead be harmful. Women end up with higher exposure to radiation for mammograms over their lifetime, which increases their chance of getting radiation-induced breast cancer that they may not have gotten otherwise.1
Most women who have a mother, sister, or grandmother who had breast cancer at the age of 50 or older, or who are at high risk of breast cancer because of obesity or other reasons, may want to have regular mammograms (every two years) starting between ages 40 and 50. If their relatives had breast cancer at a young age, women may consider mammograms even before age 40. Unfortunately, younger women tend to have denser breasts, which often look white on a mammogram. Since cancer also shows up as white, mammograms are less accurate for younger women (and other women with dense breasts). For those women, a breast MRI is likely to be more accurate than a mammogram, and they are safer than mammograms.
Breast MRIs are more expensive than mammograms, costing an average of $2,000 (compared to about $100 for a mammogram). The Task Force says there isn’t enough information to recommend for or against MRIs. For that reason, insurance may not cover the cost. If you want insurance to pay for an MRI, you probably need your doctor to recommend it because of your high risk. Women with dense breasts are at higher risk, especially women with mothers or sisters who had breast cancer at a young age. It is logical that they could potentially benefit from regular breast MRIs, but research is lacking to draw conclusions.
Which kinds of cancer risks can help me decide?
A 2011 article by Dr. John Schousboe and his colleagues published in the Annals of Internal Medicine examined mammography for women at different ages and with different risk factors.2 Biennial mammography (screening once every two years) had health benefits and was cost effective for all women 40-79 with high breast density or with both a family history of breast cancer and a breast biopsy, regardless of breast density. Biennial mammography was also beneficial for women aged 50-69 with average breast density and women 60-79 with low breast density and either a family history of breast cancer or a previous breast biopsy. Annual mammography was not cost-effective for any group.
The study’s authors concluded that each woman’s decision about mammography screening should be based on the following risk factors: age, breast density, history of breast biopsy, family history of breast cancer, and personal beliefs about the benefits and harms of screening. This study supports the Task Force guidelines that women at an average risk of breast cancer can start biennial screening at age 50 and that women at a higher breast cancer risk should consider screening before age 50.2
The chances of getting breast cancer increase with age, and the disease is much more likely after age 50 than before. So, from a public health and cost-effectiveness perspective, annual screening mammograms do the most good after age 50. Earlier mammograms are less accurate and more likely to result in unnecessary anxiety or unnecessary biopsies. Unlike Schousboe and his colleagues, the Task Force did not recommend routine screening for women 75 and older, because there was not enough evidence to conclude whether or not the benefits outweigh the risks. However, the American Cancer Society recommends that screening every other year continue for older women whose health is good enough that they are likely to live at least 10 years. That is a difficult standard to implement: How many doctors want to tell their healthy older patients that they are not likely to live at least 10 more years?
Isn’t more frequent mammography better?
Remember that mammograms expose women to radiation, which can increase the risk of breast cancer. Increasing the age of mammograms to age 50 for most women, and reducing the frequency to every two years could save lives because it would drastically reduce radiation exposure. Experts believe that less frequent mammograms also means a lower false alarm rate, and that means fewer unnecessary tests, anxiety, and possibly fewer unnecessary surgeries.34
Do mammograms save lives?
Between 1975 and 2000, dramatic improvements in treatments for breast cancer became available. Surgery options were improved, important chemotherapy agents were discovered, and tamoxifen, a hormonal treatment for estrogen-sensitive breast cancer, came into widespread use. At the same time, mammography became more popular. In 2000, about 70% of women 40 and over reported that they had a mammogram within the previous two years. Mammography rates more than doubled between 1987 and 1999, but more recently rates have decreased slightly.
The result of these important advances has been a dramatic decrease in the number of breast cancer deaths, even while more cases of breast cancer were being diagnosed. The five-year survival rate for breast cancer increased from 75% between 1974 and 1976, to 88% by 1995-2000. Have the survival rates improved because of mammography or because of better treatments?
This became a full-fledged medical controversy in recent years. Two issues were at the root of the debate: 1) was mammography simply uncovering more tiny, slow-growing cancers that would never have developed into a health threat even if they had never been discovered? and 2) were we doing more harm than good by subjecting so many women to cancer treatment without knowing whether some of these very early cancers would really become dangerous? Since 2009, research has shown that some tiny cancers disappear on their own without treatment. For example, experts now conclude that most ductal carcinoma in situ (DCIS) will never become an invasive breast cancer, even without treatment.
Regular screening mammography helps diagnose cancer earlier but the latest research suggests it may not be saving lives, except possibly for the highest risk women. Researchers estimate that for 40-year-old women, fewer than 2 lives will be saved out of 1000 women who have annual mammograms.5 During that time, approximately 600 of these 1000 women will have false alarms, and approximately 5-10 will have unnecessary surgical treatment that could be harmful to them. This latest research did not consider the benefits compared to the risks of regular mammography (every two years) after age 50. We believe that starting less frequent mammography at 50 (and for women at high risk between the ages 40 and 50) continue to provide benefits that may outweigh the risks for most women. Although about 90% of worrisome findings from mammograms turn out to be false alarms — not cancer — the overall benefits have been established for women over 50.
What about breast self-exams? The Task Force recommends against teaching women to do breast self-exams, because evidence suggests the risks outweigh the benefits. There are many “false alarms,” and by the time a cancer is large enough to be felt in a self-exam, it will soon be found anyway, in the shower or while dressing. And the Task Force and the American Cancer Society no longer recommend that doctors do breast exams on their patients, for the same reason.
For more information:
U.S. Preventive Services Task Force, Breast Cancer Screening Final Recommendations, http://screeningforbreastcancer.org
For information about insurance coverage for free mammograms: http://www.hhs.gov/blog/2016/01/11/bottom-line-mammograms-are-still-covered.html
What you need to know: Breast cancer, suicide, mastectomy, and breast implants
Diana Zuckerman, PhD
2016
Breast cancer patients often describe having a new appreciation for life, so it is important for women and their friends and family members to know that women who have breast cancer have an increased likelihood of committing suicide for up to 15 years after their cancer diagnosis 6 7.
Even more surprising, the one study of suicide among women who got breast implants after mastectomy found that their suicide rate was 10 times higher compared to other mastectomy patients 8. More research is needed, but for some reason this study has received little attention and no other studies were conducted to learn more. It is important to note that all the women in the study had early-stage breast cancer – which experts agree does not require a mastectomy. In fact, the latest research indicates that women who undergo mastectomy do not live as long as women of the same age and diagnosis who undergo lumpectomy and radiation instead.
The Bottom Line
If mastectomy is not medically necessary it is a bad choice, because cancer patients who undergo mastectomy don’t live as long as lumpectomy patients and they are more likely to commit suicide.
Read more in the article in Women’s Health Issues, and our summary of it here.
Insurance Coverage Information for Breast Implant Removal
Did you know it might be possible to get health insurance coverage for breast implant removal?
I got breast augmentation with implants. Will my insurance cover my breast implant removal?
I got breast implants after a mastectomy. Will my insurance cover my breast implant removal?
Need financial assistance to get your implants removed?
First of all, the original reason for getting your breast implants matters to health insurance companies (as well as Medicare and Medicaid).
If your implants were put in after a mastectomy and your doctor believes that removing your implants is “medically necessary,” then your health insurance is legally obligated to cover your breast implant removal. Click here to learn more about your rights under the Women’s Health and Cancer Rights Act of 1998 (WHCRA).
If the original reason for getting breast implants was for augmentation of healthy breasts, then some health insurance companies will cover your explant surgery if they consider the services to be “medically necessary,” but others will not.
What if my insurance company says that “complications from cosmetic surgery” are not included?
Don’t be discouraged. Almost all health insurance policies will not cover “cosmetic surgery” or “complications from cosmetic surgery” but don’t give up so easily. Many policies have exceptions for complications from breast implants under certain circumstances that they consider “medically necessary” or “reconstructive surgery.”
What are “medically necessary” services?
This is defined differently by different health insurance companies, and sometimes varies in different states as well.
It is important to understand that even if your doctor thinks removing your breast implants is medically necessary, the health insurance policy can refuse to pay if their policy’s definition of medically necessary is different from your doctor’s.
The most generous health insurance policies regarding breast implant removal are usually based on one of the following conditions:
- Silicone gel implants that are proven to be ruptured.
- Silicone or saline implants that are causing Baker III or Baker IV capsular contracture.
- Breast implants that are causing necrosis (death of skin or tissue).
- Breast implants that need to be removed because of infection or ALCL (a rare cancer that can develop around breast implants).
Rupture: If your implants are ruptured, you will need proof. MRIs are the best measurement of implant ruptures, but ultrasounds or mammograms may be accepted too. However, the pressure from mammography can cause old breast implants to break or leak and are not very accurate for detecting rupture, so it is much better to avoid mammography if you can.
Capsular Contracture: Breast implants are a “foreign body” and the natural response for most women is that the body forms scar tissue around the implant, inside your body, to protect your body from this “foreign invader.” This is a natural process. However, it is called capsular contracture when the scar tissue tightens or hardens around the implants. Capsular contracture can happen with either saline or silicone breast implants. It can feel slightly uncomfortable or cause debilitating pain. The mild version of capsular contracture is called “Baker I” or Baker II” (named after a Dr. Baker who devised the categories) and the most severe is called “Baker III or Baker IV.” Baker III or Baker IV breasts are hard and/or painful. Insurance companies usually only consider Baker III and/or Baker IV level capsular contracture to be a medically necessary reason for removal.
Pain: Pain caused by capsular contracture is often considered justification for insurance coverage of removal. In addition, if your implants are causing extensive pain because of nerve damage or the weight of the implants, it is sometimes possible to get your insurance company to pay for removal.
Improved health after removal: If you can prove that your symptoms have drastically improved after your breast implants were removed, you may be able to make a case that it was medically necessary to remove them in the first place. If you are no longer in pain, or are now able to return to work after being unable to work as a result of complications from your breast implants, you could make a strong case for why the implant removal was needed. However, it is always riskier to pay for implant removal and then hope the surgery will be reimbursed.
What is generally NOT considered “medically necessary”?
Unfortunately, most insurance companies do not consider any autoimmune diseases/symptoms or anxiety related to your implants to be proof that it is medically necessary to remove your breast implants. However, many women who have those symptoms also have other problems, such as leaking silicone implants or capsular contracture. So, focus on the symptoms that the insurance company cares about, not the ones that they don’t cover.
What does “reconstructive surgery” mean?
Some insurance companies will consider your breast implant removal “reconstructive surgery” as opposed to “cosmetic surgery” and therefore medically necessary when the purpose of your surgery is to treat a medical condition. This usually means that you have Baker grade III or IV capsular contracture, and/or limited movement affecting your ability to do simple tasks such as reaching above your head or combing your hair. Your breast implant removal may also be considered reconstructive if you have lumps of silicone in the breast area that interfere with the diagnosis of breast cancer.
How do I know when/if my insurance plan considers breast implant removal “medically necessary”?
To find out what your insurance plan covers, you can read through a copy of your actual policy. There are often 3 versions of your health insurance policy:
- A short summary, also called a Summary of Benefits and Coverage. This will not have the information you need.
- A description of the plan. This will have more information than the summary, will probably specify that cosmetic surgery is not covered, and may even mention breast implants specifically. However, it usually will not have the specific information you need to know if your policy will cover implant removal.
- The specific policies regarding breast implants or cosmetic surgery complications are in the “contract” that you sign when you buy health insurance coverage. This contract has all the very specific policies that you need to know about. As a customer who bought that policy, you are entitled to receive a copy online or in the mail, so you can call to ask for it. If your current insurance policy does not cover implant removal, you should shop around to look for one that does. However, that can be difficult to find out.
Persistence can make a difference! For example, Medicare denied Karen’s initial claim for breast implant removal because they concluded that explanting her ruptured silicone gel implants was not medically necessary. In her appeal, she sent copies of several insurance policies from other companies, stating that they cover surgical removal of silicone gel breast implants when they are ruptured. Medicare finally granted her coverage for her explant surgery. Karen is already feeling better than she had in months/years.
We would be happy to help you with this. To start that process, you can fill out our very short survey here: https://www.surveymonkey.com/s/KHCWGM8
What do I need from my doctor?
When the time comes to ask the insurance company for coverage, it helps if your doctor sends a letter to your insurance company detailing why removal of your breast implants is medically necessary. He/she should focus on the complications that you have that are more likely to be covered by your insurance (such as implant rupture or Baker III or IV capsular contracture). It is usually better to not talk about your other symptoms (such as autoimmune symptoms), because it will detract from what the insurance company needs to hear.
What if I have Medicare?
Your doctor should be able to call Medicare’s provider line to check if your breast implant removal surgery will be covered.
Q: My implants are silicone, they were implanted before 2007, and my insurance has denied coverage to remove my implants (or I have no insurance or Medicaid). I do not have Medicare. Can you help me?
If this is the case, you may be eligible for a financial assistance program to help you afford your breast implant removal. Please visit www.explantassistance.com and download the Notice of Interest form. If you have any questions, you can contact the Program Administrator, Jeff Condra, at jcondra@oplc.org or 205-252-6784.
What do I need to know about breast implant removal surgery?
See our article here.
Less Radical Surgery is a Healthier Choice for Women with Breast Cancer
Brandel France de Bravo, MPH and Diana Zuckerman, PhD
Updated 2017
Experts have long advised that lumpectomy patients live as long as mastectomy patients. But the latest research, based on hundreds of thousands of women, indicates that women with DCIS or early-stage breast cancer are more likely to live longer, healthier lives if they choose less radical surgery.
Four studies indicate that lumpectomy patients live longer.
In a study of almost half a million women with breast cancer in one breast, Harvard cancer surgeon Dr Mehra Golshan reported in 2016 that those undergoing double mastectomies did not live longer than women undergoing a mastectomy in only one breast.[1] On average, women who underwent a lumpectomy instead of mastectomy lived longer than women undergoing either a single or double mastectomy for cancer in only one breast.
Similarly, a study of more than 37,000 women, also published in 2016, women with early-stage breast cancer who underwent lumpectomy with radiation were more likely to be alive 10 years later, compared to women who underwent mastectomies.[2] They were also less likely to have died of breast cancer or of other causes. This was true even when age and factors that could influence survival were taken into account.
Dr. Shelly Hwang and her colleagues found similar results in a 2013 study of more than 112,000 California women who had lumpectomies to remove their early-stage breast cancer were more likely to be alive and free of breast cancer 5 years after surgery than women who had mastectomies.[3] The women had been diagnosed between 1990 and 2004 with either Stage 1 or 2 breast cancer. All of them had either a lumpectomy with radiation or a mastectomy. After surgery, their health was monitored for an average of 9 years (the women were all studied for 5-14 years). The women who had a lumpectomy and radiation tended to live longer than the women who had mastectomies, when controlling for age at diagnosis, race, income, education levels, tumor grade or the number of lymph nodes with cancer. Lumpectomy with radiation was especially effective for women who were 50 years and older with hormone-receptor positive tumors: they were 19% less likely to die of any cause during the study than women just like them who had mastectomies. Perhaps more surprising, they were 13% less likely to die of breast cancer than women just like them who had mastectomies.
In a study published in 2014, Dr Allison Kurian and her colleagues at Stanford studied 189,734 California patients diagnosed from 1998 to 2011 with early-stage breast cancer in one breast, ranging from Stage 0 (DCIS) to Stage 3.[4] The study showed that the percentage of women having both breasts when only one breast had cancer (called bilateral mastectomies) increased dramatically, but there was no advantage to that more radical approach. Instead, the women who underwent lumpectomies (removing only the cancer, not the entire breast) lived longer and were more likely to be alive 10 years after diagnosis compared to women undergoing a mastectomy. Women who had both breasts surgically removed did not live longer than those undergoing a mastectomy on one breast.
Compared to women in other countries, women in the U.S. who are diagnosed with early-stage breast cancer are more likely to remove both breasts even if only one has cancer. It is not known why bilateral mastectomy provides no medical advantage, but a study of more than 4,000 cancer patients by Dr. Fahima Osman at the University of Toronto indicates that having a healthy breast removed in addition to the breast with cancer increases the chances of medical complications.[5] Removing the healthy breast (“contralateral breast”) doubled the chances of having wound complications in the first month after surgery: from about 3% for women who had only the breast with cancer removed to about 6% for women who also had the healthy breast removed. About 4% of women who had a single mastectomy experienced some kind of complication (not necessarily wound-related) in the 30 days after surgery, compared to 8% of women who had both breasts removed. The risk of cancer in that healthy breast was already less than 1% per year unless the woman has a BRCA gene or some other very high risk factor.[6] Hormone pills such as tamoxifen or aromatase inhibitors can further reduce that already low risk.
The Bottom Line: these enormous studies of women in the U.S. and other countries make it clear that women with DCIS or early-stage breast cancer should undergo surgery to remove only the DCIS lesion or cancer, not the entire breast. The women who undergo lumpectomy with radiation usually live longer than those who undergo mastectomy or bilateral mastectomy. In addition, mastectomy patients who have breast implants are more likely to kill themselves compared to mastectomy patients without implants. Unfortunately, the fear of breast cancer and desire to “get rid of the problem” has resulted in too many women undergoing mastectomies or bilateral mastectomies that threaten their lives. Physicians and breast cancer advocacy groups need to make sure that patients understand why lumpectomy with radiation is a better idea.
For a free booklet on treatment options for DCIS, click here. For a free booklet on treatment options for early-stage breast cancer, click here.
References
- Wong, S., Freedman, R., Sagara, Y., Aydogan, F., Barry, W., & Golshan, M. Growing Use of Contralateral Prophylactic Mastectomy Despite no Improvement in Long-term Survival for Invasive Breast Cancer. Annals of Surgery. 2016 March; doi:10.1097/SLA.0000000000001698
-
Marissa C. van Maaren, et al, “10 year survival after breast-conserving surgery plus radiotherapy compared with mastectomy in early breast cancer in the Netherlands: a population-based study”. Lancet Oncol. 2016 Aug; 17(8): 1158–1170. Published online 2016 Jun 22. doi: 10.1016/S1470-2045(16)30067-5
- Hwang ES, et al “Survival after lumpectomy and mastectomy for early stage invasive breast cancer: The effect of age and hormone receptor status” Cancer 2013 April 1; 119(7); DOI: 10.1002/cncr.27795.
- Kurian, Allison W., Daphne Y. Lichtensztajn, Theresa H. M. Keegan, David O. Nelson, Christina A. Clarke, and Scarlett L. Gomez. “Use of and Mortality After Bilateral Mastectomy Compared With Other Surgical Treatments for Breast Cancer in California, 1998-2011.” The Journal of the American Medical Association 2014; 312(9): 902-914. DOI:10.1001/jama.2014.10707
-
Osman, Fahima, et al “Increased postoperative complications in bilateral mastectomy patients compared to unilateral mastectomy: an analysis of the NSQIP database.” 2013 Oct; 20(10): 3212–3217. Published online 2013 Jul 12. doi: 10.1245/s10434-013-3116-1
- National Cancer Institute. Breast Cancer Treatment (PDQ®). http://www.cancer.gov/cancertopics/pdq/treatment/breast/healthprofessional/page1

The Facts About Breast Implants
What exactly are breast implants?
Breast implants are silicone envelopes filled with a liquid or gel. They are used to increase the size of a breast or to replace a breast that was removed because of breast cancer.
Most breast implants in the U.S. are filled with saline (salt water). The envelope is made of silicone and also contains other chemicals. So even if you get saline implants, you will still have some silicone in your body.
Breast implants filled with silicone gel were approved by the FDA for the first time in 2006, but only for women ages 22 and older. The FDA has not approved silicone gel breast implants as safe for augmentation for women under the age of 22 because of safety concerns.
If implants are filled with anything other than saline or silicone, they are experimental. You are taking a bigger risk if you try them. Unless you want to be a guinea pig, don’t be fooled by stories about how they are “very popular in Europe.” They aren’t.
Breast implants vary in their surface (smooth or textured), shape (round or shaped), profile (how far it sticks out), volume (size), and shell thickness. Breast implants include an envelope or shell made of silicone, a filler, and a patch to cover the manufacturing hole.
Breast implants can break and rupture, which can cause a variety of serious health problems. Implants can break in a few weeks, a few months, or a few years, although some can last 15 years or more. According to the FDA, by the time a woman has had implants for 10 years, at least one of them has broken. So, anyone who gets implants should expect to have to replace them at least once every ten years. Many women have to replace them more often because they can cause other problems in addition to breaking, and the two implants may break at different times.
Think of it like you would think about buying a new car – usually a new car doesn’t cause problems at first, but causes more and more problems as it gets older. But some cars cause problems right away, and it’s not always possible to fix them. The difference is that breast implants are in your body, and if something goes wrong the only way to fix them is to pay for surgery. There is no way to know how long your breast implants will last or whether they will cause problems.

Before You Get Implants
Are they safe?
The FDA has approved silicone gel breast implants but only for women who are 22 or older. And because of serious concerns about safety, the FDA is requiring implant makers to study 80,000 women with breast implants for 10 years.
Saline breast implants are approved by the FDA for women over 18. Why the difference? All breast implants will eventually break and leak into the body. The FDA believes that there are more serious safety questions as well as cosmetic problems when silicone gel implants leak into the body, than when saline implants leak. That’s because saline is salt water, which is not dangerous.
The FDA has approved saline breast implants made by two manufacturers, Inamed (also called McGhan or Allegan) and Mentor. The FDA has approved silicone gel breast implants made by those same two companies, and also by Silimed. All breast implants can cause problems, but breast implants made by other companies haven’t been tested for safety and are not allowed to be sold in the U.S. If you get implants made by other companies in other countries, they may be more likely to break or cause problems.

The FDA decided that breast implants are “reasonably safe” for most women, but that women need to be accurately informed about the risks.
“Reasonably safe” does not mean safe for everyone. The FDA found that most implant patients have at least one serious complication within 3 years after getting their silicone or saline implants.
The purpose of the 10-year studies is to find out how many health problems are likely during the first 10 years that a woman has implants. Unfortunately, there have been so many problems with the studies that they are not likely to be able to answer those questions.
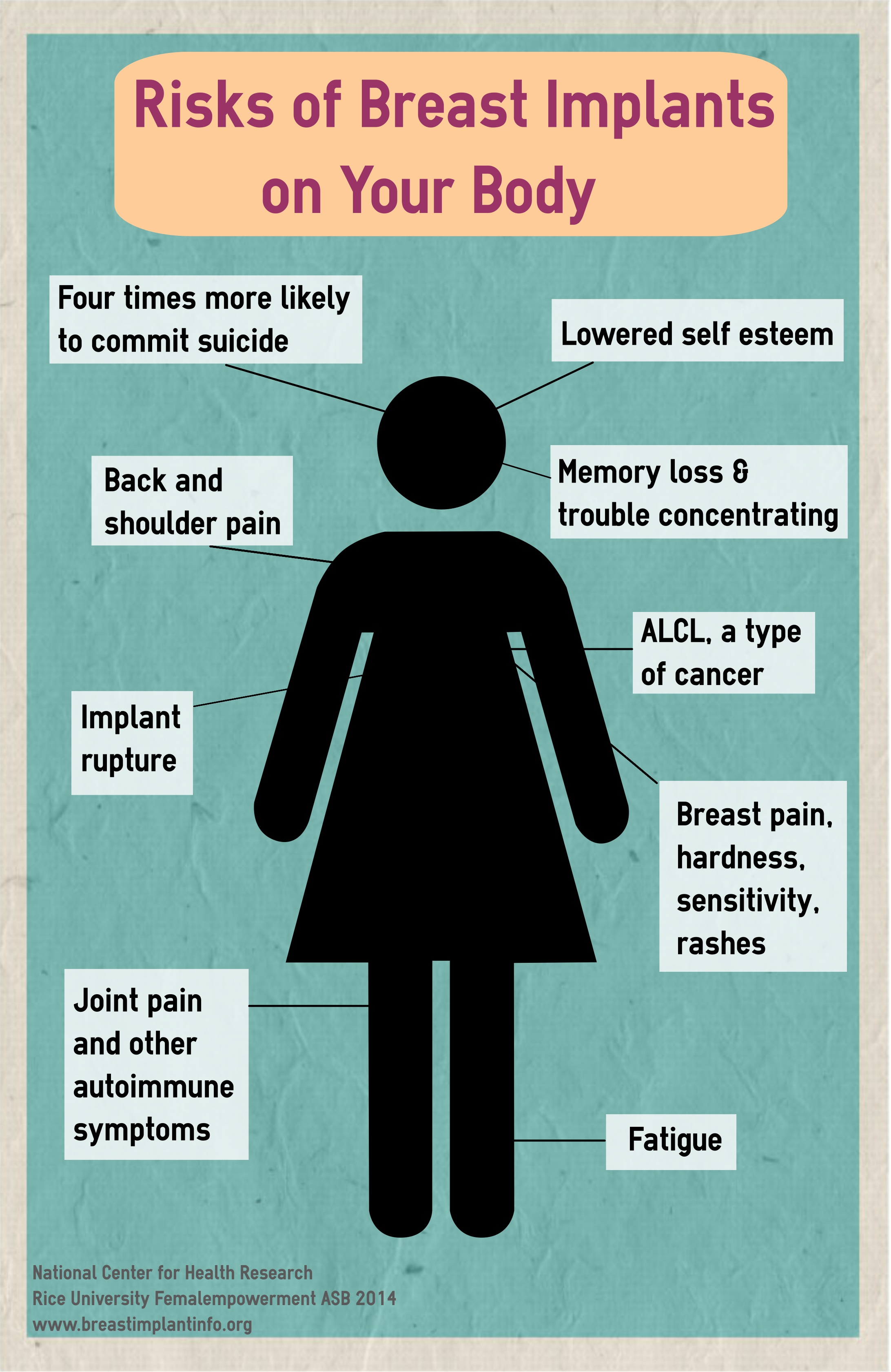
What complications should I expect?

Breast pain, breast hardness, and numbness in the nipple are common complications that may last for years, and may never go away. The most common, called capsular contracture, is when the scar tissue inside your body tightens around the breast implant. That can cause the implant to feel very hard and painful, and can make the shape look unnatural, as if you have 2 balls on your chest.
The most serious complications include toxic shock syndrome, implants breaking through the skin, or skin dying. A few studies have shown that patients have died or had gangrene as a result of breast augmentation surgery. These are rare but they do happen.
Many breast augmentation patients need additional surgery within 5 years of getting breast implants. Within 10-12 years, most women will need at least one additional surgery, and some will need 2 or more surgeries.
Complications are even more common among women getting breast implants after a mastectomy. Four out of every 10 reconstruction patients need additional surgery within three years of getting implants.
If you are thinking of having children in the future, it is important to know that breast implants may interfere with your ability to breastfeed. Breast milk is the best food for babies, so you may want to delay getting breast implants until after you are done having children.
How long do breast implants last?
It is impossible to predict how long an implant will last. Some implants break within a few days, weeks, or months, while others last for many years.
Like most new products, most implants seem fine for the first few years. Think of implants as being as reliable as a car – problems can happen anytime, but the older they get, the more problems you are likely to have, the more expensive those problems are going to be.
Eventually, you will need to get your implants replaced. A study by FDA scientists found that by the time a woman has implants for 10 years or more, at least one of them has broken.
Why do implants break?
All breast implants have the same basic design. Implants are made up of a silicone envelope, with a filling of some kind–usually either saline or silicone gel. Because of this design, all breast implants can develop a tear or hole. Whether the hole or tear is large or small, it’s called a rupture.
Ruptures can happen simply as implants age, or because of a blow to the chest, such as in a car accident or a bad fall. Tears or holes can be caused by a defective implant, by a nick from a needle during a biopsy, or even when the surgeon is closing the incision in your chest after putting the implants inside you.
Saline implants have a valve. If you have saline implants, the surgeon will place the empty silicone envelope in your chest, and then use the valve to fill the envelope with saline. If the valve is defective, or breaks, it will leak.
The pressure from mammography can cause an implant to break, especially if the implants are old or the mammography technician is not trained to work with breast implants. You should always tell the technician that you have breast implants, and make sure that he or she is qualified to perform your mammogram.
Closed capsulotomy can also cause an implant to rupture, and should never be done. Closed capsulotomy is the name for a procedure when a woman has capsular contracture and the doctor squeezes the breast very hard to try to break the scar tissue capsule. Unfortunately, the squeezing can break the implant as well as the capsule.
How much do breast implants cost after the initial surgery?
Most women pay $4,000-7,000 for their first augmentation surgery with saline implants, and approximately $1,000 more with silicone gel implants. If a doctor is charging less than that, be very cautious. Make sure he or she is a board-certified plastic surgeon and is very experienced with implants.
Experts at the FDA warn that women with silicone gel breast implants should have a breast MRI three years after getting silicone implants and every two years after that. The purpose of the MRIs is to determine if the silicone gel breast implants are ruptured or leaking, because there are often no symptoms. It is important to remove silicone implants if they are ruptured, to avoid the silicone leaking into the breast or lymph nodes. Breast MRIs usually cost at least $2,000, sometimes more.
Women with saline breast implants do not need MRIs to detect rupture because saline implants deflate when they are ruptured. That makes it obvious that the implant has broken, but it is not dangerous unless there are bacteria in the implant.
Your health insurance will not pay for breast augmentation or other kinds of cosmetic surgery. Most insurance companies will not pay for most complications or medical problems that result from breast augmentation, and they will not pay for MRIs to check for rupture. Before your surgery, check to see if your health insurance company covers complications from breast implants.
Every week we hear from women who want to have their implants removed and cannot afford to do so.
If you have to pay for breast implants on an installment plan or by borrowing money, then it is very risky to get breast implants. You might still be paying off your surgery when serious implant problems arise. It often costs more to get implants removed than to have them put in.
Do breast implants cause cancer?
Breast implants do not cause breast cancer, but they make it more difficult to detect breast cancer because they can hide tumors.
Mammograms can’t see through breast implants, and the most recent research indicates they will miss the tumors of half of the augmented women who have breast cancer.
Mammograms must be performed by a skilled technician who is aware that you have implants. This costs more, takes longer, and will expose you to more radiation each time you have a mammogram. And according to a study by FDA scientists, mammograms can cause implants to rupture.
Research by the National Cancer Institute has found that women with breast augmentation are more likely to die of brain cancer or lung cancer compared to other plastic surgery patients. However, the scientists who did the study aren’t sure whether that is conclusive or just happened by chance.
What to ask your doctor
If you decide to get breast implants put in or taken out, make sure you only use a board-certified plastic surgeon.
If your doctor shows photographs of patients, ask if they were his or her own patients. Ask to see photographs of how they looked a few years later.
If your doctor tells you that breast implants are proven safe, ask what kinds of problems can happen to women who have breast implants.
Ask your doctor for written information about the risks of breast implants and read that information at least one week before surgery, so you have time to ask questions or gather more information.
Any woman who considers silicone gel implants should ask for the informed consent form at least one week before surgery.
If your doctor says all of his or her patients are happy with their results, ask to speak to patients who have had implants for at least 7-10 years.
Legal Issues
Many women wonder why implant companies agreed to a legal settlement for billions of dollars to help women harmed by breast implants, and yet breast implants can still be sold today. To read a report summarizing these legal issues, written by the Alliance for Justice, click here.
What do the experts say about breast implants?
Well-respected women’s health expert Dr. Susan Wood and the former president of the American Society of Plastic Surgeons, Dr. Scott Spear, spell out the risks of silicone breast implants in a new article. To read a summary, click here.

How Will Breast Implants Change Your Life?
More Surgeries
You will have to get many more surgeries to either replace your old implants at least every ten years or surgery to simple remove them and try to get your breasts looking like they did before implants.
 In addition, you may need extra medical treatment or surgeries to help treat any cosmetic or medical problems caused by the implants. Implants are not a one time deal and will have to be dealt with throughout the rest of your life.
In addition, you may need extra medical treatment or surgeries to help treat any cosmetic or medical problems caused by the implants. Implants are not a one time deal and will have to be dealt with throughout the rest of your life.
Attention Grabbers
While many girls get implants to make themselves stand out more, you may not like the attention as much as you think. Guys may stare at your chest instead of looking at your face when they talk to you, and your girlfriends may be uncomfortable and awkward about your new breasts as well. Several celebrities have spoken about feeling like their breasts entered a room before they did. It may be hard to ignore their stares and comments.
Also, keep in mind that you will have to buy new clothes to fit your new body. While this may sound exciting, it can be even more challenging for a thin or average weight girl or woman to find clothes that fit bigger breasts as it was to find clothes that fit smaller breasts.
Implants will affect you forever
Whether you are happy or unhappy with your implants, implants will affect you forever. You may be completely satisfied with your implants, and satisfied when you have to replace them. But just keep in mind, that they don’t work out for everyone, and you may be left with breasts that are as hard as rocks or looking like a very elderly woman. Seriously think about if you want this kind of drastic change in your life, throughout your entire life. Immediate results are usually positive for girls, but it’s important to remember that this decision will be with you forever, so choose wisely.

Teens and Breast Implants
• According to the American Society of Plastic Surgeons, more than 226,170 teenagers underwent plastic surgery and cosmetic procedures in 2015. 9 Most were nonsurgical procedures such as laser hair removal and laser skin resurfacing, but breast augmentation was one of the most popular surgeries.
• Breast augmentation has become a frequently-requested high school graduation gift. How frequently is it requested, or given as a gift? Nobody really knows, since the research has not been done.
• Is it appropriate to perform cosmetic surgery on patients whose bodies are still maturing? Breast development can continue into the late teens and early twenties, so girls who think they need augmentation now might change their mind later.
• There are no epidemiological studies or clinical trials on the safety and long-term risks of breast implants and liposuction on patients under 18. So, the risks are unknown.
• Although the FDA approved silicone gel breast implants only for women ages 21 and older, and saline breast implants only for women 18 and older, there are no legal restrictions on the procedure. The American Society of Plastic Surgeons has an official position against breast augmentation for most teens under 18, but there is no enforcement. The American Society for Aesthetic Plastic Surgeons has no official position regarding augmentation for teenagers.
• Research has shown that of all age groups, teenagers are the most likely to be dissatisfied with their appearance — and that the dissatisfaction lessens with age. A long-term study conducted on both boys and girls ages 11-18 found that body image satisfaction was highest at age 18 for both boys and girls. In other words, older teens feel better about their bodies than younger teens.10 The study also found that the features participants were most dissatisfied with reflected the culturally determined stereotypes emphasized in books, mass media and advertisements.
• Breast augmentation has a very high complication rate that often requires additional surgery within five to ten years.11 , 12 For a girl of 18, that means she will probably need another surgery while she is in her 20s, her 30s, and every decade after that.
• Based on the implant makers’ own studies, the FDA concluded that about 40% of augmentation patients have at least one serious complication within three years after getting their implants. 4
• Breast pain, breast hardness, and numbness in the nipple area are common complications that may last for years, and may never go away.3
• According to studies by the National Cancer Institute and other researchers, breast augmentation patients are four times more likely to commit suicide compared to other women of the same age, including former plastic surgery patients of the same age.13 The risk of lung cancer and some other cancers also is higher for breast augmentation patients compared to similar women without implants.
• Health insurance usually will not pay for the necessary treatment or corrective surgeries for breast implant problems. Teens may not think about their future financial security, since their main concern is the immediate gratification of fixing a perceived problem with their bodies. But fixing implant problems costs thousands of dollars each time, so these financial considerations are important.
• Breast implants interfere with mammography, obscuring 55% of breast tumors, on average.14
• Breast implant surgery sometimes causes infections leading to toxic shock syndrome, amputation or death.15
• Women who have breast implants are less likely to have enough milk to be able to breastfeed, compared to women who have not had breast surgery. 16
• If a teenager changes her mind and has her implants removed a few years later, her breasts are likely to look stretched-out and saggy. 17 This is especially true for women with larger implants.


Are Breast Implants Dangerous?
Surgery has Risks
Like with all surgeries, you always go in knowing that something potentially could go wrong. Usually it won’t but sometimes it will, and some people have died from breast implant surgery. Risks from surgery include infection, hematoma (blood or tissue collecting around an implant), and serious complications that can happen with anesthesia. Infections are usually easy to treat, but doctors have reported that some women have gotten toxic shock syndrome from infections, and others have gotten gangrene.
The main risks from breast implants are not from the surgery itself. The main risks are what happens in the months and years after the surgery. You should keep those risks in mind while making your decision.
A few side effects…so you know how the result may turn out
• Implant surgery can cause you to lose sensitivity in your breasts, especially in your nipples. Or your breasts can become so sensitive that it is painful to be touched. Either problem may dampen sexual intimacy.
• You may suffer from capsular contracture: 
This is when scar tissue forms around the implant (because it is a foreign body), and causes your breasts to become unnaturally hard, painful, have an unnatural shape, or become lopsided.
This young woman’s breasts look unnatural and the left one is a different shape than the right because of capsular contracture.
• If you get saline implants, they could make a swishing sound that you or others near you can hear.
• Breasts with saline implants tend to feel unnaturally cool compared to real, warmer breasts.
• If you snowboard, ice skate, or play in the snow, your saline implants may feel very uncomfortably cold.
And when you’re older…
Even if you’re not concerned with the future right now, the truth is that getting older is inevitable. So, it is very important to think about any risks breast implants could give you that would affect your life in the years to come.
• Do you ever want to have kids? Breast feeding your children is extremely important to their health. Research shows that women with implants are more likely to have an inadequate supply of milk for their babies, or nursing could be painful. So if having healthy babies is important to you, you may want to delay breast implants until afterwards.
• Breast Cancer: The idea of breast cancer may not have even crossed your mind yet, but when you get older and need mammograms, implants interfere with being able to detect cancer early. Even the best mammograms will miss up to half of the breast area where cancer can grow, because it will be hidden by the implants.
Life-threatening Risks
Below is a list of what research shows about the risks of getting breast implants. Keep these dangers in mind before making your decision.
According to the National Cancer Institute, compared to other plastic surgery patients, women with breast implants are:
• Twice as likely to die from brain cancer
• Three times as likely to die from lung cancer
• Four times as likely to kill themselves
According to an FDA study there may be a link between implants and some auto-immune and connective tissue diseases. A link to fibromyalgia (which causes chronic muscle pain and severe fatigue) has also been found.
Who Should Avoid Breast Implants?
Implants are riskier for some girls and women than others. If you have had an autoimmune disease or if family members do (such as rheumatoid arthritis, lupus, or chronic fatigue syndrome), you should not take the chance of a foreign body like breast implants. If you are concerned about breast cancer, you should not get implants since they interfere with detecting breast cancer early by interfering with mammograms.
Need more facts?
The two implant companies that can legally sell saline breast implants in the U.S., Mentor and Inamed, conducted their own studies about the risks of saline implants.
If you’re considering silicone gel breast implants, read about an implant makers’ own studies of silicone gel implants here.
Some other risks to consider…
Money
Breast augmentation surgery usually costs about $4,000 to $6,000). If a doctor is charging less than that, be very cautious. Make sure he or she is a board-certified plastic surgeon and is very experienced with implants.
Paying this kind of money is not a one-time deal. You will need to spend more money to replace your implants when they break or wear out, or pay to have them removed even if you don’t want them replaced. Even if the implant is under warrantee, or if your doctor offers his services for free if problems arise, the anesthesia and other fees will still total thousands of dollars.
Health insurance will not cover breast augmentation, and usually will not pay the cost of medical care if you have problems that need to be fixed. Even if your implant breaks or is causing an allergic reaction, health insurance probably will not pay the cost of medical care. You will either have to ask your parents to pay to fix or replace the implants, or take out a loan yourself to cover the costs.
We have heard from teens and young women who arranged to pay off their augmentation on a monthly basis, but then needed to have them removed before they had finished paying for the implants themselves. Going into debt to get implants is risky. Our advice: only get implants if you can afford to have them removed if something goes wrong.
Your Looks
Almost every teenage girl is concerned with her looks, and that is obviously the reason some get implants. If breast implants gave every girl beautiful breasts for the rest of her life, that might seem like a good idea. However, augmented breasts that look natural at first, can change and look and feel much less natural and less attractive in just a few months or years. We’ve heard from celebrities who were embarrassed to be hugged because their breasts were so hard.
If you need to have your implants removed, they may look very saggy and stretched out – not nearly as good as they looked before you got implants.
That is definitely not what you want to accomplish.
What do we mean by looking unnatural? Some girls describe their “new” breasts as looking like two balls attached to their chest. Others find that one breast is much higher than it should be, or you can see or feel the implant. If the breasts look round and if there is space between the breasts instead of cleavage, those are two common signs of breast implants.
Keep in mind…
You’re still growing! Even if you’ve heard this before, it’s still true. Not only may your breasts still be growing, but the rest of your body could be too. Most teens find their breasts look more voluptuous in their early 20’s than they did in their teens, without augmentation.
Also, you may want to wait a little longer to see if you really want implants, or if you are still experiencing normal teenage self-consciousness. The truth is, the older you get, the more accepting you become of your body and the better you feel about yourself. Research on girls ages 11-18 found that girls liked their body more every year. In other words, older teens feel better about their bodies than younger teens. The study also found that the features that girls were most dissatisfied with reflected the ideal looks emphasized in books, mass media and advertisements.